GERD: From “Just Heartburn” to a Complex Digestive Disorder
For decades, heartburn was dismissed as a minor inconvenience, something you treated with an antacid and moved on with your day. But modern research tells a very different story.
Today, gastroesophageal reflux disease (GERD) is recognized as one of the most common chronic digestive disorders in the world, affecting up to 20–30% of adults in Western countries.
Scientists now understand that GERD is not simply “too much stomach acid.” Instead, it is a multifactorial condition involving anatomy, nerve signaling, digestive motility, and lifestyle factors. In other words, the story of GERD has evolved dramatically over time, and understanding that evolution helps us better treat it today.

What Is GERD?
GERD occurs when stomach contents repeatedly flow backward into the esophagus, irritating or damaging its lining.
The reason for this is NOT STRICTLY because you create too much acid, and we have to understand this to move on.
A small amount of reflux is actually normal physiology. Healthy people experience brief reflux episodes throughout the day without symptoms because the body has several protective mechanisms that quickly clear the acid.
GERD is diagnosed when reflux:
Causes persistent symptoms
Leads to inflammation or injury of the esophagus
Significantly impacts quality of life
Common symptoms include:
Burning chest pain (heartburn)
Acid regurgitation or sour taste in the mouth
Difficulty swallowing (dysphagia)
Chronic cough or throat irritation
Hoarseness or frequent throat clearing
In more severe or long-standing cases, GERD can contribute to complications such as esophagitis, Barrett’s esophagus, strictures, and even esophageal cancer.
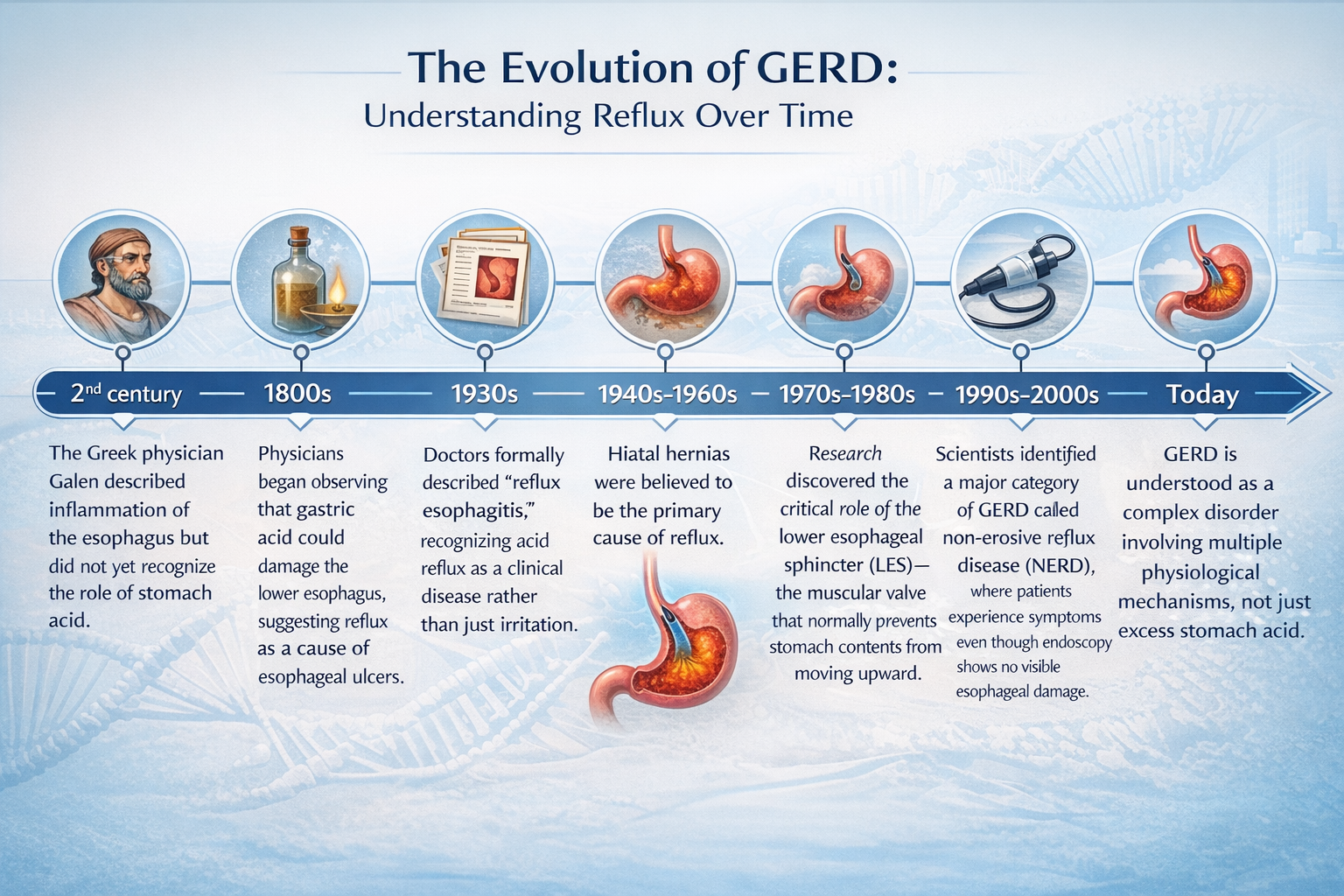
A Brief History of GERD: How Our Understanding Has Changed
What Actually Causes GERD?
The body has several natural defenses that normally prevent reflux, including:
The lower esophageal sphincter (LES) acts as a valve that, when healthy, prevents acid backflow
Esophageal peristalsis that clears acid (this is the cellular movement downwards to prevent upward movement)
Saliva that neutralizes acid
Protective mucosal lining of the esophagus
GERD develops when these protective systems are overwhelmed. Several mechanisms are now known to contribute.
Transient Lower Esophageal Sphincter Relaxations
These are short episodes when the LES relaxes temporarily without swallowing.
They occur in healthy people as well, but in GERD patients, these relaxations more often allow acid to escape into the esophagus.
2. Weak Lower Esophageal Sphincter
In some people, the LES maintains abnormally low resting pressure, allowing stomach contents to reflux more easily—especially when lying down.
3. Hiatal Hernia
A hiatal hernia occurs when part of the stomach pushes upward through the diaphragm.
This anatomical change weakens the anti-reflux barrier and increases exposure of the esophagus to stomach acid.
4. The “Acid Pocket”
Researchers have identified an area near the stomach entrance called the acid pocket—a small zone of highly acidic gastric fluid that forms after meals.
This pocket can escape upward into the esophagus, explaining why many reflux episodes occur after eating, even when food should be buffering stomach acid.
5. Delayed Gastric Emptying
If food leaves the stomach slowly (as seen in conditions like gastroparesis), stomach pressure increases and reflux becomes more likely.
Risk Factors for GERD
Both lifestyle and biological factors can influence reflux risk.
The most common include: Obesity or increased abdominal pressure, pregnancy, smoking, hiatal hernia, certain medications, dietary triggers; which are specific person to person.
Foods often associated with reflux symptoms include fatty foods, chocolate, alcohol, caffeine, and spicy meals. However, research shows these triggers can vary widely between individuals; this is where food sensitivity investigation comes into play.
GERD Is More Than Just Heartburn
Many people associate GERD only with burning chest pain, but reflux can affect multiple organ systems.
Some patients experience extra-esophageal symptoms, including:
Chronic dry cough
Asthma flare-ups
Laryngitis or hoarseness
Recurrent throat clearing
Dental enamel erosion
In fact, GERD is believed to be one of the most common causes of non-cardiac chest pain and may worsen respiratory conditions like asthma in some individuals.
How GERD Is Treated Today, Conventionally
Treatment strategies for GERD generally fall into four categories.
1- Lifestyle Modifications: These are often the first step and can significantly reduce symptoms.
Examples include:
Weight loss when appropriate
Avoiding late-night meals
Elevating the head of the bed
Identifying individual food triggers
Reducing alcohol and tobacco use
Some studies also suggest that Mediterranean-style diets and alkaline water may help reduce reflux symptoms.
2- Medications: The most common medications are proton pump inhibitors (PPIs) such as omeprazole (Prilosec), esomeprazole (Nexium), lansoprazole (Prevacid), dexlansoprazole (Dexilant), pantoprazole (Protonix), and rabeprazole (AcipHex), which reduce stomach acid production. These drugs can effectively relieve symptoms and heal esophageal inflammation in many patients. However, they do not address all the underlying mechanisms of GERD. This may explain why some patients continue to experience symptoms despite acid suppression.
3- Endoscopic Therapies: Certain minimally invasive procedures can strengthen the lower esophageal sphincter using radiofrequency therapy and endoscopic suturing techniques. These approaches are typically reserved for carefully selected patients.
4- Surgical Options: For severe or persistent GERD, laparoscopic fundoplication surgery may be performed to reinforce the anti-reflux barrier between the stomach and esophagus.
The Future of GERD Treatment
One of the most important realizations in modern gastroenterology is that GERD is not just an acid problem so determining the CAUSE is the key to healing instead of ‘bandaid’ medicine.
It is a disorder involving nerve signaling (addressing nervous system regulation), muscle function (physical therapy), digestive motility (diet and supplements often ideal to support, anatomy (understanding YOUR body), and lifestyle factors.
Because of this, future treatments will likely focus on multiple therapeutic targets rather than just reducing stomach acid.
As our understanding of GERD continues to evolve, the hope is that treatment will become more personalized, addressing the root causes driving reflux in each individual patient.
Digestive health is deeply connected to the rest of the body, and persistent symptoms like reflux should never be ignored. If you’re experiencing chronic heartburn, throat symptoms, or digestive discomfort, it’s worth exploring the underlying causes rather than simply masking symptoms.
Here to empower you with the knowledge of health,
Dr. Meg Holpuch
Disclaimer: The information provided on this blog is for educational and informational purposes only and is not intended as medical advice, diagnosis, or treatment. The content shared here is not meant to replace or supersede the guidance or recommendations of your personal healthcare provider. Always consult your physician or qualified healthcare professional before making any changes to your diet, exercise routine, supplement regimen, or overall health plan. Your health and well-being are unique, and decisions regarding your care should always be made in consultation with your trusted healthcare provider.